
Michael Shawn Harmon
Latest posts by Michael Shawn Harmon (see all)
- A Game of Numbers: Sperm Count & Semen Analysis - November 21, 2019
- Mind the Gap: Varicocele, Surgery & Gonads (Again) - November 21, 2019
- Lost in Translation: Testosterone Replacement Therapy, the HPG Axis, Infertility & Marital Stress - November 21, 2019
A semen analysis is one of the first tests conducted when you visit a fertility clinic. The results of the analysis determine if a man is producing sperm, his sperm count (total number of sperm in the total volume of ejaculated semen), his sperm concentration (number of sperm in a milliliter of ejaculated semen) and sperm/semen “quality.” I’m placing “quality” in quotation marks because its importance is questioned by some reproductive endocrinologists. More on “sperm quality” later in this post. And no, I’m not going to talk about my experiences with the collection process. It deserves its own dedicated and explicitly explanatory post. I SWEAR that I will write about it ASAP.
The Greatest Journey I’ve Never Told:
A sperm cell’s journey begins when the testes are stimulated to produce sperm and ultimately ends when a sperm cell reaches the fallopian tubes and moves in with an egg.
Immature and obnoxious sperm cells are produced in the testes. It can take 50 to 60 days for the testes to produce sperm. The immature sperm are then shuttled to the epididymis, located next to each testicle in the scrotum. The epididymis teach sperm to mature and become respectable citizens of the scrotum. This maturation process takes around 12 to 14 days. Mature sperm cells are stored in a section of the epididymis until it’s GO TIME.
So there is no misunderstanding, GO TIME is that special, special moment once per year when two people who are married (sometimes to each other) make sweet, sweet love in the missionary position in a tender, gentle and monotonous semi-stimulating manner to serve as a physical but nonverbal manifestation of their undying commitment and adoration of each other as ordained by God. Sometimes, if you’re lucky, the special moment concludes with weird facial expressions and strange noises. And then you’re done until next year.
When the most special of the special moment arrives, ejaculation is triggered and the epididymis (both of them) will release mature sperm cells (but not all of them) into the vas deferens. The vas deferens, also called ductus deferens, is connected to the section of the epididymis where mature sperm have been patiently waiting. There are two vas deferens, one for each epididymis, and are each between 30 cm to 45 cm in length. Sperm is transported by the vas deferens out of the scrotum through the spermatic cord. Once “inside” the body, the vas deferens diverges from the spermatic cord and loops over and around the bladder.
The final part of the vas deferens “tube” is called the ampulla. The ampulla contributes a small amount of fluid to support the health of sperm and acts as a reservoir system. The ampulla quickly connects with a duct from the seminal vesicle. The seminal vesicles add a lot of nutrients to the concoction (now called seminal fluid). The junction of the ampulla with the seminal vesical forms the short ejaculatory duct (insert joke here).
Remember, there are two of everything until both ejaculatory ducts release their seminal fluid into the prostatic urethra. This section of the urethra is called “prostatic” because it is surrounded by the prostate gland. The prostate gland excretes additional fluid to mix with the seminal fluid as it passes through. We can now call this mixture Semen (finally).
Almost There. Semen continues down the urethra and passes by the bulbourethral glands (sorry, there ARE two of them but they both serve the urethra). They are also called Cowper’s glands. These glands add the “pre-sperm” or “pre-ejaculate” fluid.
And then the fun stuff happens. The semen in the urethra enters the penis and, after what I’m sure is yet another impressively long journey, is ejaculated into the vagina (usually).
Semen:
Semen is the fluid ejaculated by the male body. Men typically ejaculate a total semen volume of 2 to 5 milliliters (mL). Only between 2% to 5% of semen consists of sperm. The remainder of seminal fluid is provided primarily by three accessory glands of the male reproductive system.
The seminal glands (also called seminal vesicle) produce around 60% of the fluid in total semen volume. The fluid consists mostly of fructose. Fructose provides sperm cells with the energy they need for all the laps they are about to swim. Approximately 30% of total semen volume is contributed by the prostate gland. The prostate gland contributes enzymes, zinc, citric acid, magnesium, potassium and other nutrients. The bulbourethral glands add a very small amount to total semen volume, but its contribution is very important because it lubricates the urethra and vagina.
At least 95% of the fluid in semen is dedicated to the health, welfare and general encouragement of sperm to go forth and give it their all.
Semen Analysis: What is it and how did it become what it is today?
Semen analysis, in various forms, has been around for hundreds of years. The process has become more and more standardized as medical science has progressed. A semen analysis is considered to be the cornerstone of a fertility diagnostic workup for men. Most fertility clinics adhere to the World Health Organization (WHO) reference standards in determining the “normality” of semen/sperm parameters.
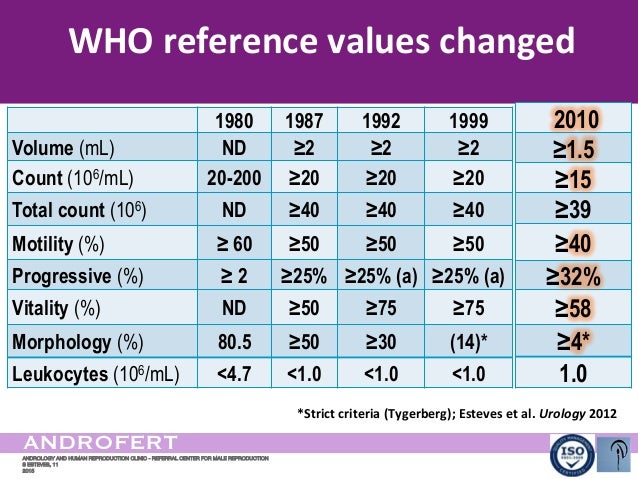
The “WHO manual for the examination of human semen and sperm[semen]-cervical mucus interaction” has been around since 1980 and the reference values for semen and sperm have changed over time. The WHO 5th Edition manual was published in 2010 and the reference values are current. Laboratories use the WHO “standard methodology” when analyzing a man’s semen. Below is a graphic showing how the WHO reference values for semen and sperm have changed over time. It includes only the minimum standards of a healthy semen analysis.
-

WHO Semen Analysis

World Health Organization semen analysis values over time
All of this sounds really confusing because it is really confusing. Just know that a man’s semen and sperm are “judged” in comparison with standards adopted by the WHO. Below is a graphic that is a little easier to understand. It includes the WHO reference range for a normal or healthy semen analysis, not just the minimum values:
| WHO reference range | |
| Total sperm count in ejaculate | 39–928 million |
| Ejaculate volume | 1.5–7.6 mL |
| Sperm concentration | 15–259 million per mL |
| Total motility (progressive and non-progressive) | 40–81 percent |
| Progressive motility | 32–75 percent |
| Sperm morphology | 4–48 percent |
World Health Organization normal value range of a semen analysis
Semen Analysis Parameters: What is measured and what does it mean?
A typical semen analysis measures sperm count, sperm concentration, sperm viability, sperm motility and velocity, sperm morphology, total semen volume, semen liquefaction, and semen pH values and leukocytes. There are more semen and sperm values examined than I have listed. Many more. But these are the usual parameters provided in a semen analysis report.
Sperm count and Sperm Concentration both refer to the number of sperm, measured in millions, in a given volume of semen. The two terms are often used interchangeably, though they do not mean the same thing. Sperm count is the total number of sperm in the total volume of a semen sample. Sperm concentration is the total number of sperm in one milliliter of a semen sample. Sperm count and sperm concentration are expressed in millions of sperm cells per a given volume of semen (sperm count = million sperm cells per total semen volume; sperm concentration = million sperm cells per a milliliter of semen). A laboratory analysis will express sperm concentration as “million/mL.”
Sperm Count the WHO standard for what is considered normal total sperm count is greater than or equal to 39 million per total semen volume. Unless a man is producing NO sperm, it is probably of little value in determining male fertility. It is only potentially significant if total semen volume is very low. “Very low” is usually measured as ejaculating less than 1 milliliter of total semen volume. According to most of the authorities that I’ve read, sperm concentration has greater predictive value.
Sperm concentration is considered by many fertility specialists to be the most important factor measured by a semen analysis. The typical man produces between 15 million to 200 million sperm cells per milliliter of semen. But these numbers can vary. Sperm concentration naturally varies from one day to the next. It also depends on when a man last ejaculated. Additionally, the competency of the laboratory performing the analysis, along with unique peculiarities endemic to the “collection process”, can also change the numbers.
A very high sperm concentration does not provide a fertility advantage. Studies indicate that there is no detectable increase in pregnancy rates when sperm concentration is greater than 40 or 50 million (one study indicates 40 and another indicates 50). A man should be shooting for (P to the U to the N) a sperm concentration somewhere between the 40 to 50 million/mL range. Some studies indicate that a sperm concentration higher than 250 million/mL can reduce a man’s fertility and increase spontaneous abortion rates, but a definitive link has not been established.
Total Semen Volume is the measure of the total quantity of ejaculated semen. It is measured in milliliters. A man typically ejaculates between 2 ml to 5 ml of semen. The total volume can vary for several reasons. Some of the reasons include the amount of time that has lapsed since he last ejaculated, whether or not all of the ejaculated semen made it to the “collection” cup, and if there were problems with the laboratory’s ability to extract semen from the collection cup. FYI: Most fertility specialists will ask a man to abstain from ejaculating for about 4 days prior to the collection date.
Sperm Motility and Velocity is a measurement of how well and how fast a sperm cell can swim. “Healthy” sperm motility and velocity is measured as forward progression of at least 25 micrometers per second. I’m not kidding. They measure this stuff. Anyway, a fertility specialist is likely to tell a man that his sperm motility is low if less than 40% of his sperm are considered motile. Some specialists indicate that sperm motility (or sperm motile density) is the most important part of a semen analysis. On the other hand, some fertility specialists consider sperm motility to be of little importance unless a man has no motile sperm.
Semen pH Values, according to the World Health Organization, semen should range between 7.1 to 8.0 on the pH scale. The pH scale ranges from 0 to 14. Since a pH of 7.0 is neutral, semen should be slightly basic (not acidic). Vaginal pH values are more important. Normal vaginal pH is 3.8 to 4.5. Cervical mucus produced during ovulation temporarily changes vaginal pH values to between 7.0 to 8.0. This change protects sperm motility and creates a safe path for sperm to travel quickly through the cervix, uterus and to the Fallopian Tube.
Semen Liquefaction is measured as the ability of semen to change from a gel to a liquid after ejaculation. The preferred amount of time is within about 15 to 20 minutes after ejaculation, but I’ve also read that up to 60 minutes may be okay.
Leukocytes are white blood cells. A white blood cell count greater than 1 million per milliliter of semen is believed to be indicative of inflammation and therefore not sponge-worthy (bonus points if you know the reference). Maybe you have a cold.
Sperm viability refers to the percentage of sperm in semen that is “alive.” Average sperm viability is around 60%, so it is not unusual for a large percentage of sperm to be DOA. Sperm viability testing may also include an analysis of sperm that is alive but have certain defects precluding fertilization. This can include testing for sperm DNA fragmentation (SDF); a determination of a sperm cell’s ability to deliver undamaged DNA.
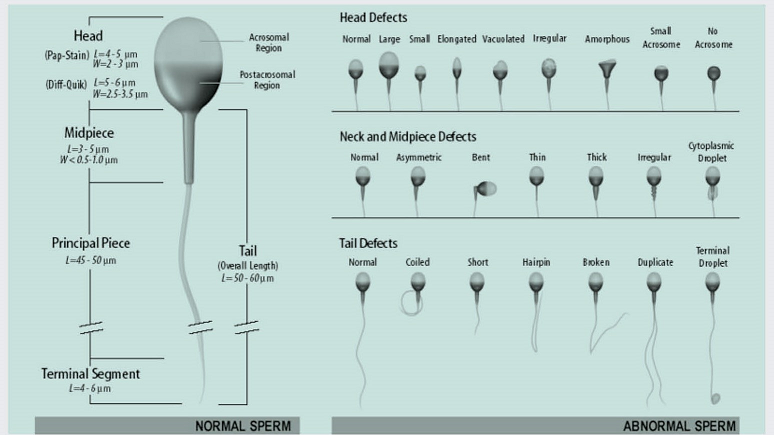
Sperm Morphology is a beauty contest for sperm cells. They are judged on their size, shape, and knowledge of current geopolitics. Sperm morphology as a predictor of reproductive outcomes is measured using Kruger strict criteria (also called Tygerberg strict criteria). Kruger criteria is named after a physician in South Africa who worked at Tygerberg Hospital and believed very strongly that using the best looking sperm to artificially fertilize an egg led to the best reproductive outcomes (Kruger criteria).The WHO adopted the Kruger strict criteria and considers anything less than 4% “normal” morphology to be indicative of male infertility that may require the use of ART (IVF, IUI, etc.).
The following are the strict criteria requirements that must be found for a sperm cell to be considered normally formed:
- a smooth rimmed, oval shaped head
- a head that is between 2.5 to 3.5 micrometers (μm) wide and 5 to 6 μm long
- an acrosome (a membrane with enzymes capable of penetrating the egg’s membrane) tip that covers between 40 and 70 percent of the sperm head
- a head free of large vacuoles (fluid filled organelles) and have no more than two small vacuoles that take up less than 20 percent of the total head
- midpiece of the sperm (the segment between the head and tail) should be about the same length as the head but much slimmer
- an uncoiled, 45 μm-long tail that should be thinner than the sperm head and midpiece
- free from head or tail defects[1] Normal Sperm Requirements
-
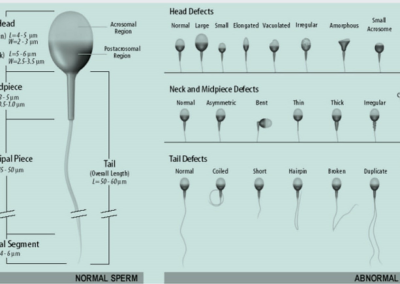
Sperm Morphology
{kind=link}
Sperm Morphology Normal and Abnormal
{kind=link}
How and what do they use to measure this stuff? A microscope and a sextant (Not going to say it. Too easy).
The Trials and Tribulations of Sperm Morphology: Is it important or not?
Opinions on the importance of sperm morphology as it relates to male fertility are all over the map. The “look” of sperm cells has been assessed for over 30 years to evaluate a man’s fertility. The belief that sperm morphology can be used to diagnose a man’s potential fertility persists: Importance of sperm morphology, Sperm morphology has high predictive value for male fertility when correctly evaluated, Sperm morphology fundamental component of semen analysis when using new evaluation technique. However, the most recent studies seem to have reached a consensus that sperm morphology is of little predictive value in assessing male fertility: Men with complete absence of normal sperm morphology exhibit high rates of success without assisted reproduction, Current evidence suggests sperm morphology has low predictive value for pregnancy success for both natural and assisted reproduction, Clinicians should base ART decisions on factors other than sperm morphology and Morphology of sperm is non-informative.
Postscript:
What to believe about all this (especially sperm morphology)? I certainly cannot and am not qualified to answer that question. My advice is to discuss the varied opinions on the parameters measured in a semen analysis with your medical provider. I wish that I could be of more help but the science is still evolving on this topic. Also, I’m an attorney. I’ve never been remotely close to a medical degree. I’m not even sure what one looks like. I’d keep that in mind, too.
[1] https://www.medicalnewstoday.com/articles/318963.php#sperm-morphology-tests
Recent Comments