
Michael Shawn Harmon
Latest posts by Michael Shawn Harmon (see all)
- A Game of Numbers: Sperm Count & Semen Analysis - November 21, 2019
- Mind the Gap: Varicocele, Surgery & Gonads (Again) - November 21, 2019
- Lost in Translation: Testosterone Replacement Therapy, the HPG Axis, Infertility & Marital Stress - November 21, 2019
Varicocele is the leading cause of infertility in men. As much as 40% of infertile men have varicocele. Varicocele is common and is also very treatable. Treatment usually requires a medical procedure. Varicocele repair is successful over 90% of the time.
What the hell is a Varicocele?
Think of varicocele like a varicose vein, but in a man’s scrotum. Isn’t that a great mental picture to start your day? Arteries and veins (and other stuff) are supplied to the testes by the spermatic cord. It is suspected that varicocele is caused when valves in the veins of the spermatic cord fail to work properly and blood flow becomes impeded. Poor circulation eventually causes blood to “back up” and enlarge the veins in the scrotum. In other words, blood flows into the scrotum (arteries) but has trouble pumping out (veins). And the condition is nothing new. The first written description of varicocele was documented 2,000 years ago by a Greek philosopher named Cornelius Celsus. There’s no practical reason for you to know that, but I thought it was cool (Pun . . . stay tuned) and decided to throw it in.
This collection of enlarged or dilatated veins in the scrotum can often be easily seen, especially when standing (because, gravity). They are rarely found in both testicles but a varicocele in only one testicle can negatively impact the function of both. Varicocele is colloquially described as appearing or feeling like a “bag of worms” upon examination by a member of the medical community, or whomever you use to check your balls. Varicocele most often develops during puberty.
The severity (size) of a varicocele is graded on a scale from 0 to III (there is no symbol for the number “0” in the Roman Numeral System; whoever created this scale was drunk). The least severe is a subclinical grade of “0” and most severe is graded a “III.”[1]
-
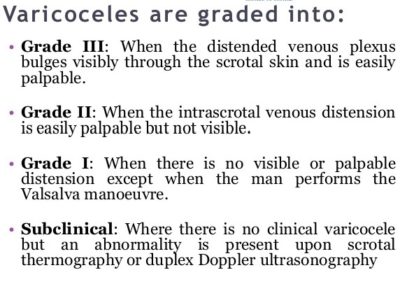
Varicocele Grade

Varicocele Grade Subclinical (0) to Grade III
The condition is typically isolated to the left testicle. The left and right testicle each have a separate system of veins to carry blood out of the scrotum. These two systems are developmentally and anatomically slightly different from each other. The valve system (seriously) of the left testicular veins have a very annoying tendency to stop working properly, resulting in a varicocele.

Left and Right Testicle venous drainage anatomy
Varicocele is very common. Between 15% and 20% of the adult male population have varicocele. While it is the primary cause of infertility in men, varicocele only rarely leads to infertility. About 85% of men with varicocele are fertile. So, a substantial majority of men with varicocele have no issue having children and rarely notice or think of it as a potential problem. However, even in fertile men, varicocele can lower testosterone levels as well as sperm production and quality. And these negative impacts on testicular function are also believed to be progressive.
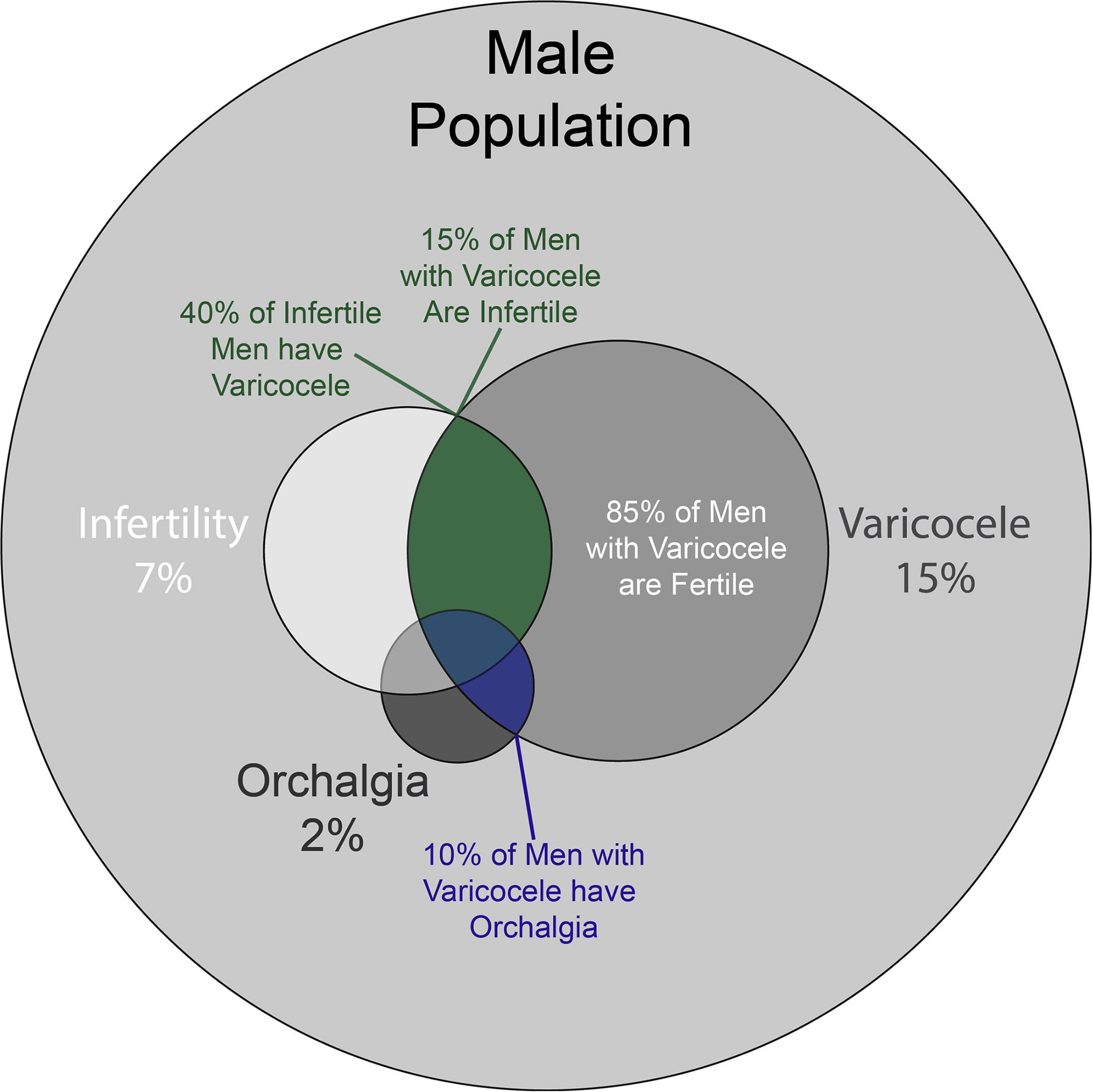
Varicocele and the Male Population
How does Varicocele impair Fertility?
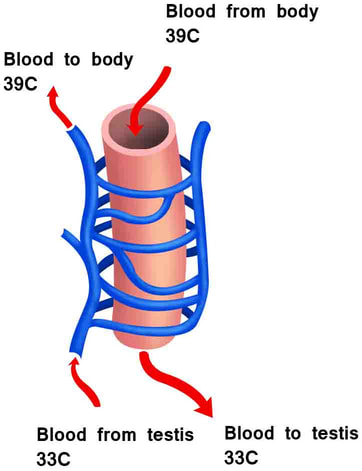
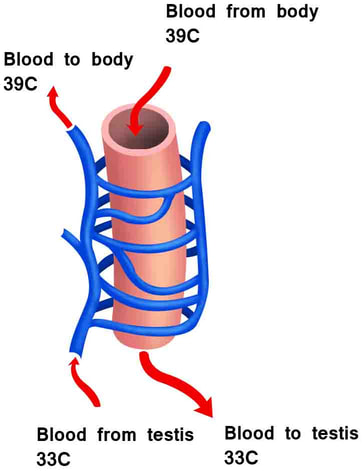
Scrotal Hyperthermia, a/k/a “Hot as Balls Syndrome” (that’s a joke, people) is believed to be a primary culprit. There’s a reason that the testes hang-out in the scrotum and not “inside” the body. The production of sperm and testosterone are very sensitive to temperature. The ideal temperature for testicular function is somewhere around 95°F or 35°C (though some authorities believe it should be cooler and others say it should be warmer). Suffice it to say that the testes should be several degrees cooler than the core body temperature of 98.6°F or 37°C.
Other than residing “outside” of the body, there are other mechanisms at work that attempt to maintain the testes at the ideal temperature. Muscles in the scrotum will relax (to cool the testicles by keeping them farther from the body) or contract (to warm the testicles by bringing them closer to the body) to maintain ideal temperature.
Another mechanism requires proper blood flow in and out of the scrotum. It is theorized that a “heat exchange” system between arteries and veins above the testicle is critical to cooling the testes. A varicocele screws up this cooling system. Blood flow out of the scrotum is impaired and collects in veins of the scrotum. The heat exchange above the testes is impaired and may result in an increase in the temperature of the scrotum. The increased temperature can impair the ability of the testes to produce testosterone and impair sperm production and quality.
-
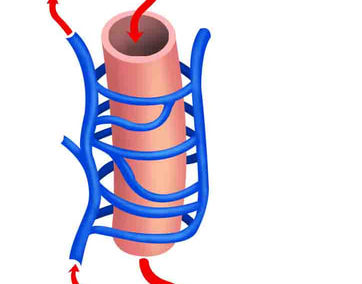
Heat Exchange
Heat stress is not the only potential cause of impaired fertility associated with varicocele. There are other, less established theories as to how a varicocele relates to impaired testicular function. These theories revolve around stagnant or decreased blood flow in the testicle. Impaired blood flow can inhibit the ability to effectively clear the accumulation of free radicals leading to oxidative stress that can damage sperm DNA. That’s not good. Similarly, stagnant blood flow may cause hypoxia (inadequate oxygen supply) in the tissues of the testicle. The resulting tissue damage diminishes sperm production and sperm quality. That’s not good, either.
Treatment Options:
Most men with varicocele do not seek and may not need any treatment. Varicocele repair has typically been recommended only when it is a suspected cause of infertility (or impaired fertility) and/or scrotum pain (often described as a dull ache but reported by less than 10% of men with varicocele).
These recommendations may soon change. As stated, the data suggests that the negative impact of varicocele on testicular function may be progressive. And an increasing number of studies suggest that varicocele repair should be considered earlier, before a man’s fertility is potentially impaired. Recent studies and published articles also indicate that the long-term negative effects of varicocele can impact a man’s overall health and is not limited only to his fertility and testosterone production.
There are several treatment options available for the repair of varicocele. The goal of each type of treatment is to block, shut off or remove the veins feeding the varicocele and thereby negate impaired blood flow believed to be the cause of the enlargement of veins in the scrotum. In most cases, the varicocele will diminish following treatment to the point that it is no longer detectable.
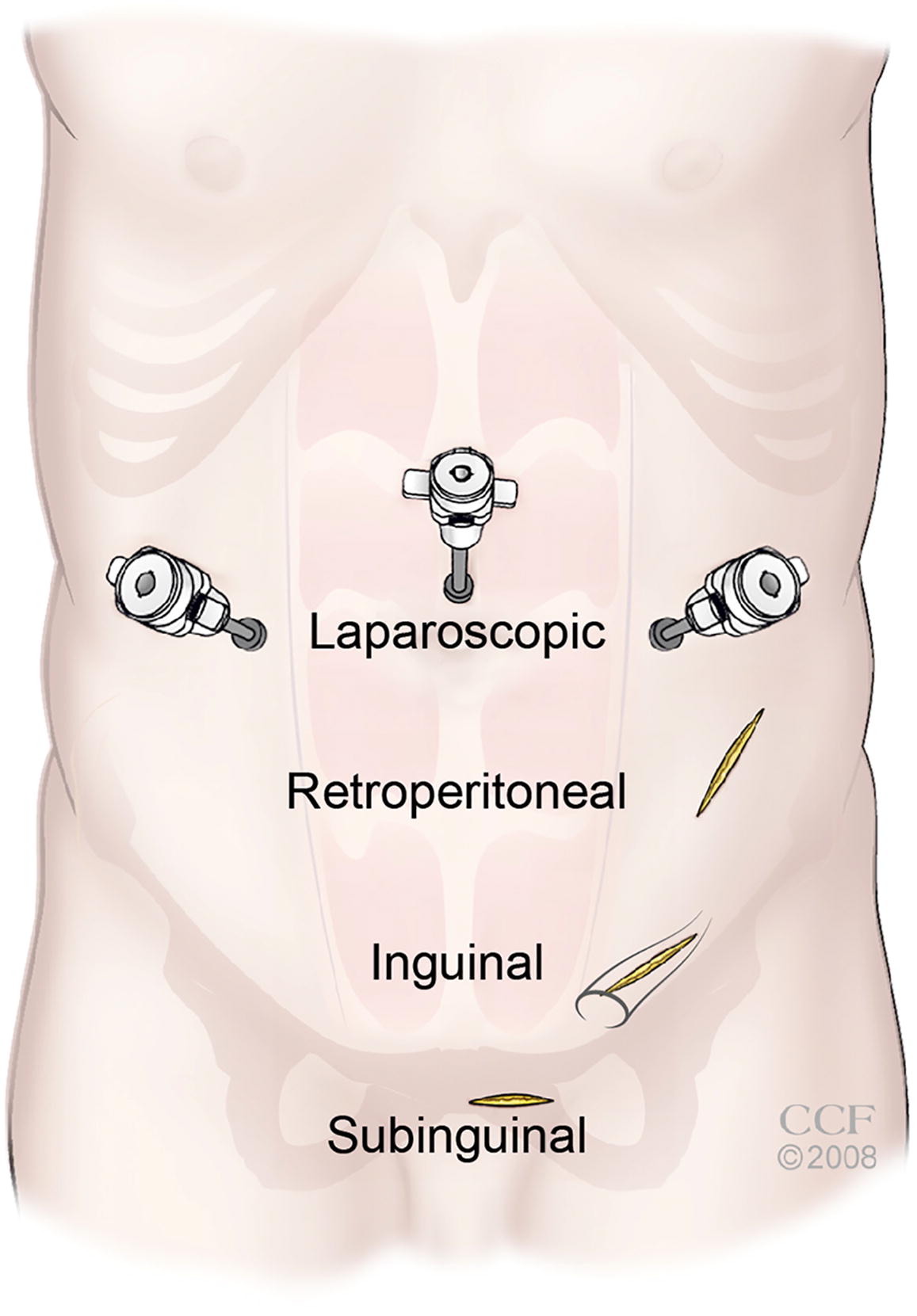
Treatment options range from procedures that require no incision, to procedures that require a few very small incisions in the abdomen and/or groin (laparoscopic), to open surgical techniques that require a larger incision in the groin. Some surgeries involve a varicocelectomy (the offending veins are removed) and other techniques involve “exposing” the spermatic cord as well as the testicle in order to “more easily” examine and repair the varicocele. The good news is that varicocele repair is usually an out-patient procedure.
{kind=link}
{kind=link}
{kind=link}
Varicocele Surgical Approach Locations
{kind=link}
None of these options sound very fun (they aren’t) and there is always a very low risk of a complication, such as cutting or tying-off the wrong thing. So, don’t allow your dental surgeon anywhere near your nuts. Instead, call the people who decided to use their M.D. to focus on the male urinary tract and disorders of the franks & beans. This causes me to wonder if Urologists’ mock Proctologists or if it’s the other way around? [P.U.N.]
Any who, an open surgical technique called “microsurgical subinguinal varicocele ligation” is performed by many urologists for varicocele repair. I do not know if there is “preferred” method. The recommended treatment option is highly dependent on the facts and circumstances of each person. I suspect that the chosen technique also depends on the desired outcome (to increase T production, improve sperm parameters, to stop pain caused by the condition or all the above). Successful varicocele repair is achieved a high percentage of the time regardless of technique. Specific treatment outcomes are more difficult to interpret.
Specific Treatment Outcomes:
The efficacy of specific varicocele repair outcomes is a bit muddled. Researching its effectiveness involves the study of many different and often conflicting statistical analyses as well as wadding-through and deciphering the conclusions of varied studies. The normal bickering betwixt authors of “competing” medical research articles can make it very difficult to elucidate precise findings for specific outcomes. The disagreements of these scholars tend to boil down to the authors of one published study accusing the authors of an earlier published study of “doing it wrong.” But, that’s the scientific method. I think.
Here’s what I believe I know about specific outcomes after varicocele repair:
- Testosterone serum levels in all men will usually increase[2] or maybe not[3];
- Testosterone serum levels increase more dramatically for men who presented with below normal T levels as compared with men who presented with T levels in the low-normal range[4];
- Pain reported by men with varicocele is resolved 80% of the time[5];
- Semen quality uniformly improves for men who presented with a clinically significant varicocele[6];
- Sperm concentration improves more dramatically for men who presented with a grade II or III varicocele[7];
- Spontaneous pregnancy rates (not assisted) increased, including in men who initially presented as infertile[8];
- Subclinical varicoceles (a “0” on the grading scale, only detected via ultrasound, least severe) appear to have no significant correlation with a man’s fertility[9];
- Results may vary between different repair techniques.
And that’s all I’ve got to say about that.
DRUM ROLL . . .
And now it’s time for my gonads to make their appearance:
I’m very sorry for the mental image I may have created, but there is no easy or gentle way for me to openly talk about my balls and their brief encounter with varicocele surgery. [Yes, we’ve returned to talking about gonads. This is not unusual for men. We’ve talked about our gonads, using much more inventive words, for most of our lives. I suspect that this is not the case for most women and their gonads.]
As you may know, my ability to produce testosterone and sperm returned after I stopped testosterone replacement therapy. The “quality” of my sperm, I was told, was not where it needed to be to achieve a high probability of natural or spontaneous fertilization. There will be much more on the efficacy of sperm “quality” as it correlates to male fertility in my next post.
I met with a urologist who specialized in male infertility to see what my options were, if any. That’s when I learned about my varicocele (left nut only) and its connection with fertility. Also, my varicocele was given a grade! I believe it was graded between a (Roman Numeral) I and II.
My varicocele was repaired using the microsurgical subinguinal varicocele ligation technique. The surgery was performed under general anesthesia. It took around 30 to 40 minutes and involved a one-inch incision in my lower left groin. The spermatic cord was isolated and the veins responsible for the varicocele were ligated (tied-off). It’s more complex than I’ve described, obviously, but that’s the gist of it.
I returned to work a few days after surgery and shuffled around very, very slowly and very, very carefully. There is some pain involved but it is not remotely comparable to the much more intense and longer-lasting pain of orthoscopic surgery on a knee, shoulder or elbow (I’ve had all of them). I was mostly concerned with avoiding unexpected impacts to my groin (as opposed to the expected ones?) and that everything stayed in place as much as possible. Also, no sex for several weeks and it would be about 6 months before I could take a fertility test and have my testosterone levels rechecked.
It takes the body time to heal and, like stopping TRT, to adjust to changed conditions. Also, sperm production and maturation are not a fast process. It takes a man an average of 60 to 70 days to produce mature sperm cells. That’s actually much longer than it takes a woman’s body to produce a mature ovum or egg. The difference, of course, is that women are born with their lifetime supply of oocytes (what will mature into an ovum or egg during ovulation) and men are not born with sperm cells (not even the immature and sarcastic ones). The production of the male gamete starts from scratch.
My Results:
At last, we’ve reached the point where I let you know that my testosterone production, sperm production and sperm quality all improved. The improvements were good but not dramatic. Mild numbness radiated from the surgical incision and into my left scrotum for at least two years. It has since resolved with no further complications. There is no doubt in my mind that I would repeat varicocele surgery if I were given the choice to start all over again.
Most importantly, the improvement was enough to increase the chance of my wife and I becoming pregnant naturally and without any assisted reproductive technology (ART) medical procedures.
Spoilers:
A natural pregnancy would have avoided the “assistance” of physicians, nurses, lab technicians, sonographers, sample collectors, plastic cups, ancient Hustler magazines, hypnotherapists, acupuncturists, massage therapists, nutritionists [I’m far from done], herbalists, a masticating juicer[10], stacks of supplements, organic farmers, folk healers, a local wise woman, Krista Tippett podcasts (Ben Greenfield podcasts for me[11]), stacks of books and their authors, parents, other people’s parents, support groups, mindfulness gurus, countless meditation masters and retreats, yogis, artificial intelligence, iPhone apps, strangers on Facebook message boards, friends, the friends of friends, Christians, former Christians, reformed Christians, priests, pastors, wiccans and a monk.
All the above were consulted or employed by one or both of us at some point while trying to conceive through artificial means (Except, ironically, artificial intelligence. But the wiccans are true). And I’m leaving out a slew of other people and things. My contribution to the list is very limited, though Testosterone Replacement Therapy withdrawal and Varicocele Surgery is not insignificant. In all fairness, when medical science provides no solutions a person can become willing to try almost anything.
That covers the first one-and-a-half to two years of my marriage and our efforts to conceive.
CITATIONS:
[1] https://www.hopkinsmedicine.org/health/conditions-and-diseases/varicocele
[2] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5182225/
[3] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5936617/
[4] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5182225/
[5] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6305863/
[6] https://www.hindawi.com/journals/aandrol/2015/432950/
[7] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5936617/
[8] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5922188/
[9] https://www.researchgate.net/publication/325204713_The_Effect_of_Subclinical_Varicocele_on_Pregnancy_Rates_and_Semen_Parameters_a_Systematic_Review_and_Meta-Analysis
Recent Comments