
Michael Shawn Harmon
Latest posts by Michael Shawn Harmon (see all)
- A Game of Numbers: Sperm Count & Semen Analysis - November 21, 2019
- Mind the Gap: Varicocele, Surgery & Gonads (Again) - November 21, 2019
- Lost in Translation: Testosterone Replacement Therapy, the HPG Axis, Infertility & Marital Stress - November 21, 2019
Who wants to talk about the Hypothalamic-Pituitary-Gonadal (HPG) axis? No one? Neither do I, but:
(1) It’s part of my story, and;
(2) You should be aware of its role in infertility.
The CliffsNotes version of this post is that thou shalt not partake of Testosterone Replacement Therapy (TRT) if you are a man and desire to remain fertile and have children. Full stop. Period. The End.
As an aside, do CliffsNotes still exist? Somebody let me know. I don’t want to embarrass myself in front of the Millennials.
TRT & Me: A Brief Summary
I was diagnosed with low testosterone several years before I married. I was prescribed a topical gel that was meant to “supplement” and raise the baseline level of my testosterone as measured in my blood serum. I applied the gel to my shoulders almost every morning after I showered. My physician tested my “T” levels very regularly. It climbed into the “normal” range where it remained until I stopped TRT after the first half-year of my marriage. I will discuss the particulars of my TRT experience in a later post. The specifics are not very relevant to the subject at hand. The subject at hand being: DON’T DO IT IF YOU WANT CHILDREN: TRT is a Male Contraceptive[1]
The Fertility Clinic:
My wife and I decided to begin trying to have children fairly quickly after marriage. My wife and her first husband were unable to conceive, and they endured two failed IVF attempts. It was a psychological trauma for her, as I’m certain it was for him as well. My focus, therefore, was on her wellbeing. I prayed that we could conceive naturally, without the need for IVF or any other assisted reproductive technology (ART) procedures. I did not want her to relive her previous experience.
We visited a fertility clinic after six months of failing to get pregnant the fun way. A semen analysis is the most common fertility test for men and one of the first tests administered. [Again, unfortunately for you there will be much more on this “process” later]. Its purpose is to determine if male infertility is a factor in a couple’s inability to become pregnant.
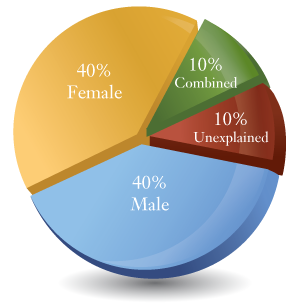
Bonus: Male infertility is a factor in approximately 40% of all cases where a couple has been unable to conceive.
-
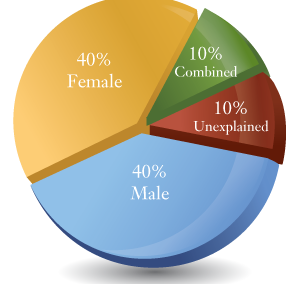
Infertility - Causes
I sat in the physician’s office as she explained that my semen analysis indicated that I was not producing sperm. NONE. My wife was with me. I had no words for her or the physician. I was confused and disoriented. I slid lower in my chair in a stunned, unreckonable daze. My first conscious thought was “Things just became a lot more complicated and challenging.” I was embarrassed. I wanted to apologize to my wife. She was already concerned about her ability to carry a child. And now, THIS. Christ, what a mess.
As our meeting continued, the physician learned that I had been using TRT for several years. With a look of relief on her face, she stated that TRT was the most likely cause of my infertility and that there was a favorable chance that my sperm production would return after cessation of TRT. But it would not return immediately (if at all) and the “quality” of my sperm could be an issue. I was advised to wait six to nine months after stopping TRT before being rechecked. If my fertility returned, it was likely going to take my body that amount of time to reboot my reproductive system.
An unexpected request by my wife:
My wife approached me one evening a few days after we learned that we would need to wait six to nine months before knowing if my gamete production returned. She had in hand a typed document that she had created. She began reading it to me. From it, she elucidated her reasons why we should consider a sperm donor instead of waiting to see what my results would be.
Her request was unexpected. Very. Unexpected. I had just learned that I was not producing sperm and I was still coming to terms with that fact. I had taken solace in knowing that there was a high likelihood that my fertility would rebound and that we would know in a relatively short time period.
I wanted children at least as much as she did. Children that I wanted to have with her. In short, my answer was “no.” I mention this episode only to illustrate the stress and anxiety that infertility can have on a marriage. We were both stressed, anxious and uncertain of our ability to have children. But we forged ahead with determination.
-
Equal
Segue:
All that we could do was wait. In the meantime, I learned a little more about what I had inadvertently done to my body and the complexity of the hormonal balance required for the reproductive system to function properly.
Sex Hormones! Gonads! Medical Terms!
The use of “exogenous” (originating externally) testosterone completely screws-up the ability of a man’s body to produce “endogenous” (originating in your body) testosterone. The ability of a man’s body to produce sperm (spermatogenesis) will also shut down and he will learn a new word called “azoospermia” (when his semen contains no sperm).
To begin, let’s talk about sex [exciting!] . . . hormones [not exciting]. Sex hormones are produced primarily by the sex glands. The sex glands are in the primary sex organs called the gonads.
The male gonads are the testes. The female gonads are the ovaries. Testosterone is the primary male sex hormone. Estrogen and Progesterone are the primary female sex hormones. The testes are responsible for producing testosterone and sperm and the ovaries are responsible for producing estrogen, progesterone and the process of ovulation.
Men also produce estrogen and progesterone, though in lower amounts than women. Women produce testosterone, though in lower amounts than men (around 5% to 10% of the amount produced by men). All these hormones and many more play a vital role in women and men for normal sexual function and reproduction. The systemic balance of sex hormones in the human body is delicate, complex and not fully understood.
THE HPG AXIS:
The HPG axis is integral to human reproduction and the expression of many of our sex hormones. The HPG axis exists in both women and men. My description of the HPG axis is very truncated and simplistic, just like me.
Let’s stop thinking about our gonads for a paragraph or two and focus instead on the hypothalamus and the pituitary gland.
The hypothalamus is an almond-sized part of your brain. Think of it (pun) as the area of the brain where your nervous system and the hormones of your endocrine system get together and communicate. Among other things, it sends messages to the pituitary gland and tells it what to do. So, the hypothalamus is pretty important.
Below the hypothalamus sits, oh so innocently, the pea-sized pituitary gland. The pituitary gland releases hormones that tell most of your other hormone-producing glands what to do. The gonads are one the hormone-producing glands that the pituitary gland orders around. So, the pituitary gland is pretty important.
A man’s gonads produce testosterone and make sperm. So, we KNOW that our gonads are damn important. A woman’s gonads produce estrogen, progesterone and store and release eggs on a periodic basis. I’m sure women know how important their gonads are but are not as abrasively braggadocious about it as men. The gonads are continually sending a report back up the chain of command to the hypothalamus and the pituitary gland to let them know that they are doing as they are told.
And that is the hypothalamic-pituitary-gonadal axis; three pretty important parts of our body that, in descending order, tell each other what to do and, more often than we would like, confuse the hell out of each other.
But wait, there’s more:
The HPG axis is a cascading loop of hormonal communication. You can also imagine it as a looping hiking trail that follows a river downstream to a confluence with an “oxbow” that circles back to the trailhead. Or maybe that’s just me. Moving on.
The release of sex hormones and the commencement of the reproductive system begins when GnRH (Gonadotropin-releasing hormone) is released by the hypothalamus. GnRH follows a pathway to the Anterior lobe of the Pituitary Gland.
Don’t worry about the posterior pituitary gland. This is already more complicated than it needs to be.
GnRH stimulates the pituitary gland to produce and release two hormones into the bloodstream: FSH (Follicle-stimulating hormone) and LH (Luteinizing hormone). FSH and LH travel to the gonads where they bind with their respective hormone receptors.
-
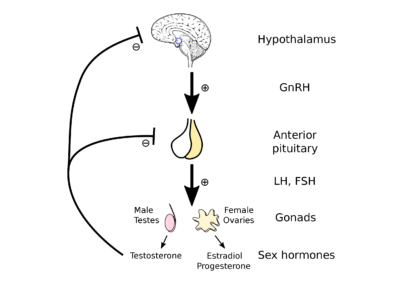
HPG AXIS - Female & Male Simplified
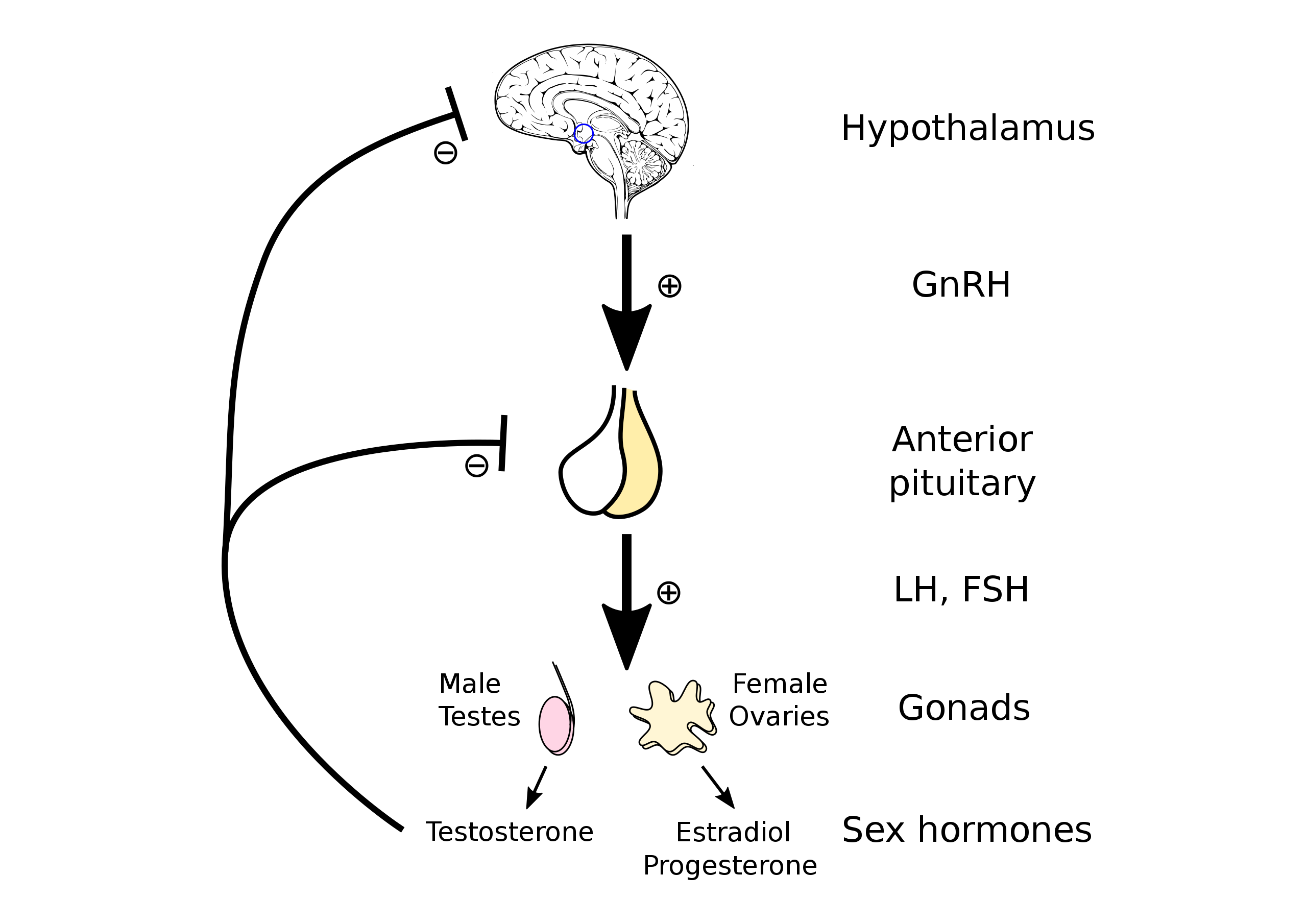
https://commons.wikimedia.org/wiki/File:Hypothalamic%E2%80%93pituitary%E2%80%93gonadal_axis.svg
In Men: FSH binds to a receptor in the Sertoli cells located in the testes. The Sertoli cells are stimulated to produce Sperm and release the hormone Inhibin. LH binds to receptors in the Leydig cells located in the testes. The Leydig cells are stimulated to produce testosterone.
In Women: FSH binds to receptors in the Ovarian Follicles and signal the follicles to begin growing. A select number of Ovarian follicles are stimulated each cycle to grow and develop oocytes (an immature ovum or egg). Typically, one follicle becomes dominant. This is the follicle that will produce and release a mature ovum or egg; the female gamete.
LH binds to receptors in the Theca Cells of Ovarian Follicles. LH and FSH work together to stimulate ovulation. A “surge” in LH further develops the ovarian follicles and stimulates the release of a mature ovum or egg. LH and FSH also stimulate the release of estrogen, progesterone and inhibin by the ovaries.
THE LOOP:
A portion of the hormones that are created by the gonads are released into the bloodstream. I say “a portion” because these hormones do a lot of things and in many different parts of the body. For instance, it is normal for a man’s gonadal testosterone levels to be 50 to 100 times higher that of the testosterone levels in the bloodstream.
One of the many things that the gonadal hormones do is report back to the hypothalamus and pituitary gland via the bloodstream. The hypothalamus will increase or decrease the release of GnRH depending on the hormonal balance, or imbalance, in the body. For men, the more testosterone that is detected the less GnRH will be secreted by the hypothalamus. The same is true of the pituitary gland and the release of FSH and LH. Our bodies seek homeostasis via this “negative feedback loop.”
How things go horribly wrong:
Let’s use me as an example. My use of TRT “tricked” my hypothalamus into believing that my testes were producing plenty of testosterone. As a result, it produced less GnRH. The decreased amount of GnRH took a short trip to my pituitary and told it to slow down the production of FSH and LH. The decreased amount of LH traveled to my testes and told them to slow down the production of testosterone. The decreased amount of FSH, combined with the decreased amount of testosterone produced by my testes, slowed my production of sperm.
And on and on it went. My hypothalamus and pituitary gland continued to “pump the brakes” on my testosterone production because they sensed that my “T” levels did not need to go any higher. My testes were continually told to slow the production of testosterone. My endogenous testosterone production eventually dropped so low that my ability to produce sperm ceased.
My use of TRT hijacked the finely tuned HPG axis and eliminated my gonads from the equation. (That sounds like an awful way to describe it, but it was an awful experience so I’m going to keep it). The “H” and the “P” thought that they were receiving accurate reports from the “G” when, in reality, they were receiving only the false report of the “TRT.” I hope that makes sense. If it doesn’t, go watch the most recent Dave Chappelle special on Netflix. You’ll understand.
-
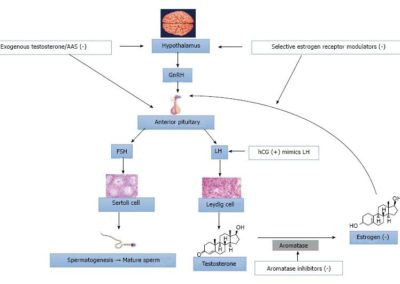
Exogenous Testosterone and the HPG Axis

{kind=link}
Exogenous Testosterone and the HPG Axis
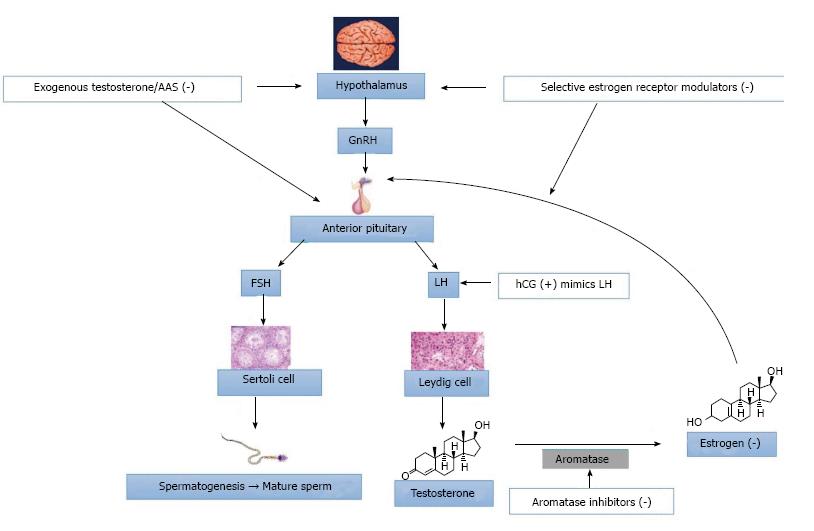{kind=link}
My Results:
I have no idea when I stopped producing sperm while using TRT and I will never know. A blood serum test can provide data that may give you a hint that your fertility is impaired but submitting to a fertility test is the only way to know with certainty.
I waited between six to nine months (I do not remember exactly how long) after I stopped using TRT to have another fertility test (semen analysis). Thankfully, my ability to produce sperm had been restored but the “quality” of my sperm was not ideal.
That’s when my wife and I consulted with another physician and agreed that varicocele surgery would be the next stop on our journey to try and procreate.
Recent Comments